
About chronichypoparathyroidism
Role of parathyroid hormone
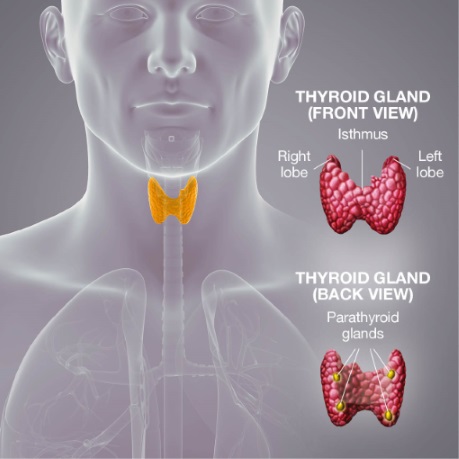
Parathyroid hormone has a variety of critical physiological functions that include its central role in modulating serum calcium and phosphate concentration within tightly regulated levels, regulating renal calcium and phosphate excretion, activating vitamin D and maintaining normal bone turnover.1
Parathyroid hormone is normally produced by the parathyroid glands, which are located on the back of the thyroid gland, in the neck (see figure).
Chronic hypoparathyroidism results in impaired mineral homeostasis*,1,2
Chronic hypoparathyroidism is a rare endocrine disease resulting from an inappropriately low circulating parathyroid hormone concentration.3
Chronic hypoparathyroidism may be defined as hypocalcaemia and insufficiently low circulating parathyroid hormone levels persisting for more than 6 months’ duration, usually following a surgical procedure.3
*In particular, calcium and phosphate.
Compromised endogenous parathyroid hormone may disrupt normal mineral homeostasis1,2,4
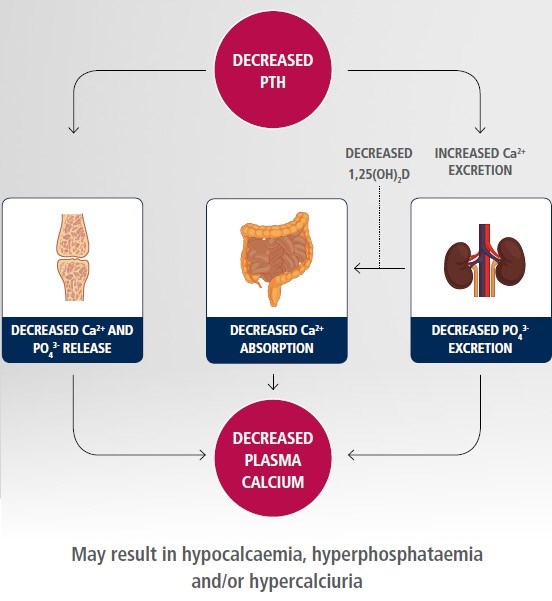
Adapted from Shoback et al. 20162 and Levine 20034
1,25(OH)2D: active vitamin D.
The impact of chronic hypoparathyroidism
Chronic hypoparathyroidism can have a substantial impact on patients’ lives:
- In a US survey conducted in 2012, patients reported the occurrence of physical, emotional and cognitive symptoms, with 72% experiencing >10 symptoms in the preceding 12 months.5
- In the same survey, hypoparathyroidism-associated symptoms and comorbidities translated into 79% of patients reporting hospital stays or emergency department visits due to their condition.5
- Chronic hypoparathyroidism is also associated with elevated risks of long-term complications, including renal and intracerebral calcifications, kidney stones, chronic kidney disease and neuropsychiatric diseases.3,6,7
Chronic hypoparathyroidism can lead to a wide range of symptoms3,5
Symptoms of chronic hypoparathyroidism were assessed in the web-based PARADOX patient survey, an online self-reported questionnaire of 374 adult US residents with chronic hypoparathyroidism.5 Patients with chronic hypoparathyroidism receiving treatment reported an average of 16 different symptoms in the previous year and experienced symptoms for an average of 13±9 hours/day.5
Symptoms can affect physical, cognitive and emotional functioning, resulting in:
- impaired mood, well-being and quality of life5,8–10
- impact on employment status and work productivity5,8
- negative effect on social life and relationships.5,8
Symptoms experienced by patients with chronic hypoparathyroidism in the last 12 months5
Adapted from Hadker et al. 2014.5 Symptoms experienced by ≥30% of patients are presented.
References
- NATPAR Summary of Product Characteristics.
- Shoback DM, Bilezikian JP, Costa AG, et al. Presentation of Hypoparathyroidism: Etiologies and Clinical Features. J Clin Endocrinol Metab 2016;101(6):2300–12.
- Bollerslev J, Rejnmark L, Marcocci C, et al. European Society of Endocrinology Clinical Guideline: Treatment of chronic hypoparathyroidism in adults. Eur J Endocrinol 2015;173(2):G1–20.
- Levine MA. Normal mineral homeostasis. Interplay of parathyroid hormone and vitamin D. Endocr Dev 2003;6:14–33.
-
Hadker N, Egan J, Sanders J, et al. Understanding the burden of illness associated with hypoparathyroidism reported among patients in the paradox study. Endocr Pract 2014;20(7):671–9.
- Mitchell DM, Regan S, Cooley MR, et al. Long-term follow-up of patients with hypoparathyroidism. J Clin Endocrinol Metab 2012;97(12):4507–14.
- Underbjerg L, Sikjaer T, Mosekilde L, et al. Cardiovascular and renal complications to postsurgical hypoparathyroidism: a Danish nationwide controlled historic follow-up study. J Bone Miner Res 2013;28(11):2277–85.
- Astor MC, Lovas K, Debowska A, et al. Epidemiology and health related quality of life in hypoparathyroidism in Norway. J Clin Endocrinol Metab 2016;101(8):3045–53.
- Arlt W, Fremerey C, Callies F, et al. Well-being, mood and calcium homeostasis in patients with hypoparathyroidism receiving standard treatment with calcium and vitamin D. Eur J Endocrinol 2002;146(2):215–22.
- Sikjaer T, Moser E, Rolighed L, et al. Concurrent hypoparathyroidism is associated with impaired physical function and quality of life in hypothyroidism. J Bone Miner Res 2016;31(7):1440–8.
Natpar® (parathyroid hormone (rDNA)
Detailed Safety Information
Please consult the Natpar Summary Product Characteristics (SmPC) before prescribing.
Natpar treatment should be supervised by a physician or other qualified healthcare professional experienced in the management of patients with hypoparathyroidism. The goal of treatment is to achieve calcaemic control and to reduce symptoms. The optimisation of parameters of calcium phosphate metabolism should be in line with current therapeutic guidelines for the treatment of hypoparathyroidism. Prior to initiating and during treatment with Natpar confirm that 25-OH vitamin D stores are sufficient and that serum magnesium is within the reference range.
Contraindications
Natpar is contraindicated in patients with hypersensitivity to the active substance or to any of the excipients, who are receiving or who have previously received radiation therapy to the skeleton, with skeletal malignancies or bone metastases, who are at increased baseline risk for osteosarcoma, with unexplained elevations of bone-specific alkaline phosphatase, with pseudohypoparathyroidism.
Warnings and Precautions
Monitoring of patients during treatment: pre-dose and in some cases post-dose serum calcium levels must be monitored during treatment with Natpar.
Hypercalcaemia: this was reported in clinical trials with Natpar. Hypercalcaemia commonly occurred during the titration period, during which doses of oral calcium, active vitamin D, and Natpar were being adjusted. Hypercalcaemia may be minimized by following the recommended dosing, the monitoring information and asking patients about any symptoms of hypercalcaemia. If severe hypercalcaemia develops, hydration and temporarily stopping Natpar, calcium and active vitamin D should be considered until serum calcium returns to the normal range. Then consider resuming Natpar, calcium and active vitamin D at lower doses.
Hypocalcaemia: a common clinical manifestation of hypoparathyroidism was reported in clinical trials with Natpar. Most of the hypocalcaemic events occurring in the clinical trials were mild to moderate severity. The risk for serious hypocalcaemia was greatest after the withdrawal of Natpar. Temporary or permanent discontinuation of Natpar must be accompanied by monitoring of serum calcium levels and increase of exogenous calcium and/or vitamin D sources as necessary. Hypocalcaemia may be minimized by following the recommended dosing, the monitoring information, and asking patients about any symptoms of hypocalcaemia.
Concomitant use with cardiac glycosides: Hypercalcaemia of any cause may predispose to digitalis toxicity, monitor serum calcium and cardiac glycoside levels and patients for signs and symptoms of digitalis toxicity.
Severe renal or hepatic disease: Natpar should be used with caution in patients with severe renal or hepatic disease because they have not been evaluated in clinical trials.
Use in young adults: Natpar should be used with caution in young adult patients with open epiphyses.
Tachyphylaxis: the calcium-raising effect of Natpar may diminish over time in some patients. The response of serum calcium concentration to administration of Natpar should be monitored at intervals to detect this and the diagnosis of tachyphylaxis considered.
Urolithiasis: Natpar has not been studied in patients with urolithiasis. Natpar should be used with caution in patients with active or recent urolithiasis because of the potential to exacerbate this condition.
Adverse Reactions
The most commonly observed adverse events with Natpar treatment were hypercalcaemia, hypocalcaemia, headache, diarrhoea, vomiting, paraesthesia, hypoaesthesia and hypercalciuria.
|
Very common
(frequency ≥1/10): |
Hypercalcaemia, hypocalcaemia, headache, hypoaesthesia, paraesthesia, diarrhoea, nausea, vomiting, arthralgia, and muscle spasms. |
|
Common
(≥1/100 to <1/10): |
Hypomagnesaemia, tetany, anxiety, insomnia, somnolence, palpitations, hypertension, cough, upper abdominal pain, muscle twitching, musculoskeletal pain, myalgia, neck pain, pain in extremities, hypercalciuria, pollakiuria, asthenia, chest pain, fatigue, injection site reactions, thirst, anti-PTH antibody positive, blood 25-hydroxycholecalciferol decreased, vitamin D decreased. |
Material code: pi-00658
Date of Preparation of SI: February 2019
Prescribing Information
| Body weight (kg) | Volume to be injected (mL) |
|---|---|
| 38–41 | 0.xx |
| 42–45 | 0.xx |
| 46–49 | 0.xx |
| 50–53 | 0.xx |
| 54–57 | 0.xx |
| 58–61 | 0.xx |
| 62–65 | 0.xx |
| 66–69 | 0.xx |
| 70–73 | 0.xx |
| 74–77 | 0.xx |
| 78–81 | 0.xx |
| 82–85 | 0.xx |
| 86–89 | 0.xx |
| 90–93 | 0.xx |